")
Developmental Pharmacodynamics (PD) constitutes the study of age related maturation of the structure and function of various organ systems and how this impacts pharmacologic response. The cellular and physiologic processes are same across mammals and yet while pharmacologic response may be the same in adults and children, the magnitude of response may not be. The response may vary due to the presence or absence of receptors, receptor binding affinity, density, and signal transduction or, in some cases, altered downstream responses. Developmental PD may impact both efficacy and safety, though in the present blog we are gauging efficacy.
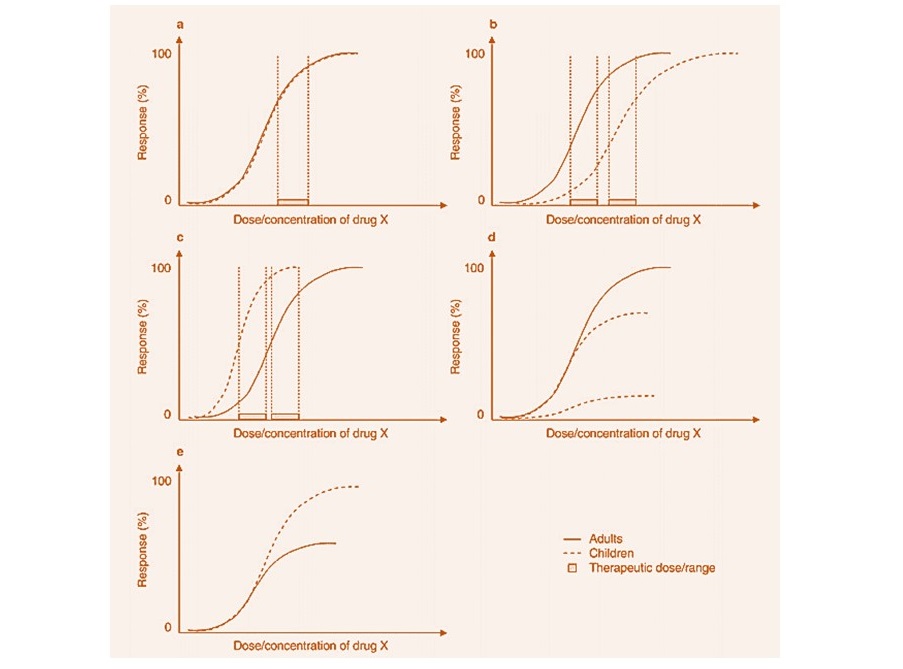
The pharmacologic response is presented above for both adults and children: on the x axis is the dose/concentration/exposure of a drug; on the y axis the response as a % of the maximum response (Emax). The dose/concentration at half the maximal response is referred to as EC50. The pharmacologic response may manifest as a change in potency (EC50) or efficacy (Emax).
Graph a: The concentration response curve for adults and children is identical. This is true for a majority of drugs. If the disease in adults and children is similar then this allows for a full extrapolation.
Graph b, Decreased Potency: The exposure response in children has shifted to the right i.e. higher EC50, thereby demonstrating reduced potency in children. In order to get the same response as in adults, one needs to target a higher exposure in children. Thus, children seem to require a higher dose of digoxin partly because of developmental changes in Na-K ATPase isoform expression.
Graph c, Increased Potency: The graph depicts increased potency in children (decreased EC50). Calcium stores in the neonatal heart are reduced compared to adults. Neonatal cardiac contractility is, therefore, more sensitive to calcium channel blockage than in adults. Calcium channel blockers are more likely to result in life-threatening hypotension in neonates. Neonates may also be more sensitive to morphine than adults, due to increased expression of the mu opioid receptor.
Graph d, Reduced Efficacy: Graph depicts a decreased Emax. In children, the lack of effect of tricyclic anti-depressants is probably due to delayed maturation of the norepinephrine system.
Graph e, Increased Efficacy: Graph depicts an increased Emax. Similar doses of warfarin in children as adults result in lower concentrations of prothrombin in children than in adults.
An understanding of the primary and secondary pharmacology of the drug and developmental PD allows for a better study design in children.
For an overview on pediatric drug development, please read our blog Pediatric Drug Development: Four Critical Considerations
Reference:
Mulla H. Understanding developmental pharmacodynamics: importance for drug development and clinical practice. Paediatr Drugs. 2010 Aug 1;12(4):223-33
For more blogs, please visit: https://www.rxmd.com/insights